







Obesity Risk Factors
What are the associated obesity risk factors? For all life on the planet Earth, except for us, food is not a choice.
Milos Pokimica
Written By: Milos Pokimica
Medically Reviewed by: Dr. Xiùying Wáng, M.D.
Updated June 9, 2023The obesity epidemic.



What are the associated obesity risk factors? Animals eat impulsively because they are conditioned to do it for survival. For all life on the planet Earth, food is not a choice. It is a daytime job of survival. The hardest thing for an animal in the wilderness is to gain weight. There is no overabundance in nature because as soon as there is, the number of animals will increase and the new balance will be achieved. This will again create a situation of constant hunger.

However, in a modern technologically driven society, there is no scarcity. This is the reason why the hardest thing for us is to diet. For most of our evolution, we were slim in a state of constant hunger as any other animal. This was the case for all of our ancestor species and that means the time period of 50 million years. The obesity epidemic today is a maladaptation that is caused by the overabundance of food. This is the new normal and the old normal of dying from starvation is a thing of the ancient past. The problem is that ”ancient” is not really ancient in evolutionary terms. Evolution works for millions of years. The obesity epidemic is therefore more than just a cosmetic issue. It is a health issue that we have to cope with and as a consequence, we will have risk factors that will be associated with it. Being overweight is not a cultural acceptance issue it is a health issue that will never be going to go away.
What are the associated obesity risk factors? The body fat percentage (BFP) measures the total fat that you have. Body mass index measures total mass depending on tallness and are different from Body fat percentage. If we have greater muscle mass or larger bones, we will have a higher BMI, so it tells us nothing about fat percentage.

For example, there is the so-called “skinny fat” body type, where you have a high BMI and high BFP or in other words, you are obese and at the same time, you have low muscle mass. Or you can have a high BMI and low BFP like bodybuilders do. Body fat percentage in the leanest athletes is typically at levels of about 6–13% for men or 14–20% for women, this means full six-pack abs and a general shredded look.

Also, there is something called visceral fat, and that is fat that we cannot see. The fat we may be capable of touching on our arms and legs is subcutaneous fat. This internal visceral fat encloses essential organs like the liver, heart, and kidneys and is called organ fat, intra-abdominal fat, or visceral fat. When you are overweight you have more fat inside than you might think. In essence, if we are obese we will have more fat inside than outside. A growing belly can be the result of both types of fat.
Carrying a large quantity of visceral fat is associated with stroke, heart disease, insulin resistance, osteoarthritis, gout, sleep apnea, asthma, breast cancer, and colorectal cancer. Individuals with a body mass index (BMI) of 30 or higher are considered obese. The term obesity is used to describe individuals who have a weight that can start to cause them health problems and is significantly above their ideal healthy weight. The term morbid obesity is used for individuals that have problems in their regular daily activities due to excessive weight gain. It is a form of disability. Nearly 70% of American adults are either overweight or obese.

Excess weight may increase the risk for many health problems, including:
- Type 2 diabetes
- High blood pressure
- Heart disease and strokes
- Certain types of cancer
- Sleep apnea
- Osteoarthritis
- Fatty liver disease
- Kidney disease
- Pregnancy problems (high blood sugar, high blood pressure)
When we talk about risk factors associated with obesity we mean only the diseases that exercise weight is going to create just by itself. In reality, the situation is very different because people that are obese usually at the same time have a very unhealthy diet. It is possible to gain a lot of weight on a nutritionally optimized whole food diet but in reality, extracted sugar and fat and other refined products make a big chunk of calories that creates the excessive caloric intake in the first place.
Having excessive weight in a more realistic condition also means having high cholesterol, high saturated fat, low mineral, low vitamin, low phytochemical and antioxidant, and high pro-inflammatory nutrient-deprived diet. Most of the people that read this will have a hard time understanding that we have in reality a situation where most obese people are also malnourished at the same time. In nutrition, there is a term “junk food” or “empty calorie”. It is similar to the “skinny fat” phenomenon.
Nutrition deficiency affects most of the population at the same time when the population is overweight. Nutritional deficiencies are a wide topic, especially because the land that is used to produce food is depleted and which means that crops will be depleted and that means that animal feed will be deleted. On top of that food is refined and the end result is hypercaloric addictive food filled with calories and nothing much else. In situations where obese people want to go on a calorie-restricted diet and are already malnourished and deficient in most of the essential and non-essential nutrients, we could have a situation that will create a wide range of diseases and all of that diseases will not be directly correlated to obesity but in a sense they are. Eating organic food has much less to do with pesticide residues or with genetically modified organisms but much more to do with low quality eroded land where these food are grown. In organic farming using synthetic fertilizers is forbidden.
Heart disease and stroke.

Besides carrying large amounts of visceral fat hypercaloric diet also in practice means a higher load of nutrients that our body is also not adapted well to metabolizing. A good example of this is cholesterol. In herbivore species, because they do not eat meat the cholesterol is produced by the liver and they do not need to eat it for their entire life. But when we start to overeat then our body will not be able to metabolize it and that will create additional deposits on blood vessels that will create an increase in risk factors from cardiovascular disease. Obesity on top of that independently just by weight creates increasing pressure on the heart muscle. The increased pressure and all of the cholesterol deposits then create pressure in small or for that measure even larger blood vessels that can be clogged. This will then lower the blood flow and as a response body will increase pressure to increase flow or some of the organs can be left without blood supply. An increase in pressure and deposited fat on the lining and inflammation then can lead to cascading bad effects. Stroke for example is the same disease as a heart attack with a different outcome. Obesity will create a higher risk of stroke. There are actually two main types of stroke, ischemic stroke, and hemorrhagic stroke. In the first one, there will be clogging of the artery and in another type, the artery will burst open. Both of them are associated with obesity.
Excess estrogen, low testosterone, and low growth hormone.

Adipose tissue is not a dead organ that sits there and does nothing. It is actually an active organ that has enzymes and is metabolically active. For example, fat cells have enzymes that will metabolize testosterone into estrogen. The enzyme is called aromatase. In breast cancer or in bodybuilding for example one of the goals is to reduce estrogen by blocking its conversion from testosterone by taking aromatase inhibitors. Testosterone is produced at the first instance and only then this enzyme changes it to estrogen. Both are very important hormones and the body needs them both. Unnaturally high levels of fat deposits will create an unnatural level of estrogen and will lower testosterone and that will have cascading effects on the rest of the body (Ylli, 2022).
It is a condition known as hypogonadism (low testosterone) and it usually comes with old age. One of the longevity treatments for the elderly is something known as testosterone replacement therapy which puts the testosterone levels in the elderly in a range of young adults. This can help with muscle wasting, libido, energy and motivation, bone density, and so on. Having low testosterone for both genders is something everyone will want to avoid.
One of the effects will be an increased risk of cancers that are estrogen-responsive such as breast cancer (Picon-Ruiz et al., 2017).


Also, higher estrogen has a wide range of cascading bad effects for itself. One would be polycystic ovarian syndrome. Having disrupted and out of balance levels of androgenic hormones is not just a question of having acne or bodybuilding. It is a serious health issue that affects the quality of life and can create serious diseases.
Disruption in androgenic hormones will also increase infertility (Pasquali et al., 2007). Obesity is associated with subfertility and more than 40% of women seeking obesity surgery do that primarily because they want to have a baby. Infertility in obese patients is correlated to androgen hormone excess on top of insulin resistance (King et al., 2013).
Fat tissue will also suppress the production of growth hormone (Scacchi et al., 1999). Growth hormone deficiency influences a person’s height and helps build bone and muscle. The growth hormone also affects metabolism (the rate at which we burn kilojoules for energy) and will burn fat at a higher rate. One of the strategies of professional athletes is to take a growth hormone to burn fat and build muscle. As for longevity treatment in the elderly, it can also help with a wide range of issues just by itself. A low level of growth hormone can cause a decrease in muscle mass and strength, very low energy levels, reduced bone density, elevated triglyceride levels, and cholesterol, it will affect collagen production and will create dry and thin skin and balding, anxiety and depression, decrease in sexual function.
Fatty liver disease.
Obesity is associated with a spectrum of liver abnormalities, known as nonalcoholic fatty liver disease (NAFLD). Most NAFLD patients are asymptomatic on clinical presentation, even though some may present fatigue, dyspepsia, and dull pain, a general feeling of being unwell and vague discomfort. Treatment for NAFLD involves weight reduction through lifestyle modifications, anti-obesity medication, and bariatric surgery. It is estimated that 75% of obese individuals are at risk of developing a simple fatty liver. A simple fatty liver is far from a “simple” condition. Up to 23% of obese individuals are at risk of developing fatty liver with inflammation. Almost 10% of children may have NAFLD, due in large part to an alarming increase in childhood obesity. In morbidly obese individuals number is 95%. In the picture, you can see how fat goes internally into the cells of the organs. The liver is swollen due to exercise fat intake. In this case, it is done deliberately by force-feeding with a tube. The practice is known as gavage.


There is also a “spillover” effect where fat cells after a point could not keep all the fat inside them and the fat leeches out to the bloodstream (Almandoz et al., 2013). Fat will then interfere with insulin signaling inside the cells and will increase the resistance of the cells to insulin creating diabetes type 2. Higher blood sugar levels will also suppress growth hormones (Møller et al., 1991). Lipotoxicity also at the same time has the ability to directly kill insulin-producing cells in the pancreas and increase the risk of diabetes type 1 (Engin, 2017).
Joint problems (osteoarthritis).

Unlike muscle tissue, the cartage is unable to adapt to the ever-increasing load of weight to the same extent. Cartilage cannot grow to become more resilient because in that case the movement would be obstructed. The consequence is that when we have an ever-larger increase in weight gain that is not congruent with our evolution there is a line where the joints are going to take severe damage in time (King et al., 2013). Obese people will have higher pressure on cartilage and it will wear down over time. There is no difference between being forced to carry bags of cement or being forced to carry excessive fat tissue. There will be physical damage. Then when cartage wears down the inflammation will start or in other words osteoarthritis. Symptoms will include pain, tenderness, swelling, stiffness, grating sensation, and loss of flexibility. This is on top of the loss of flexibility that just excessive weight will cause. In cases of morbid obesity, some people are unable to leave the bad and are unable to stand on their own and this is because of weight on top of any issues that might exist due to arthritis. Osteoarthritis is not an autoimmune disease like rheumatoid arthritis and it is caused just by physical damage to the joints. It is the most common form of arthritis. And it is a “one-way street”.
Sleep apnea.

Excessive pressure will also put a lot of strain on muscle tissue that is responsible for breathing and at the same time will obstruct breathing pathways. The narrowest part of that pathway is in the back of our throat and while we are awake that pathway is relatively open. But when we go to sleep the muscles relax and excessive weight will put pressure on them. That will cause closing by narrowing of the opening. This will interrupt breathing and will lower our oxygen intake basically this is a form of suffocation. This can cause not just snoring but interrupted sleep patterns, cardiovascular disease, and premature death. Especially if there is a combination with some other disease that causes swelling like allergies for example or smoking or taking sedatives. Most of the people that are obese have this to some extent and the real problem is that a big chunk of people will have this for a long time before they realize that they have it. When you’re awake, muscles keep. But when you sleep, those muscles relax, allowing the opening to narrow. In Western countries prevalence is estimated at around 2% of women and 4% of men (Schwartz et al., 2008).
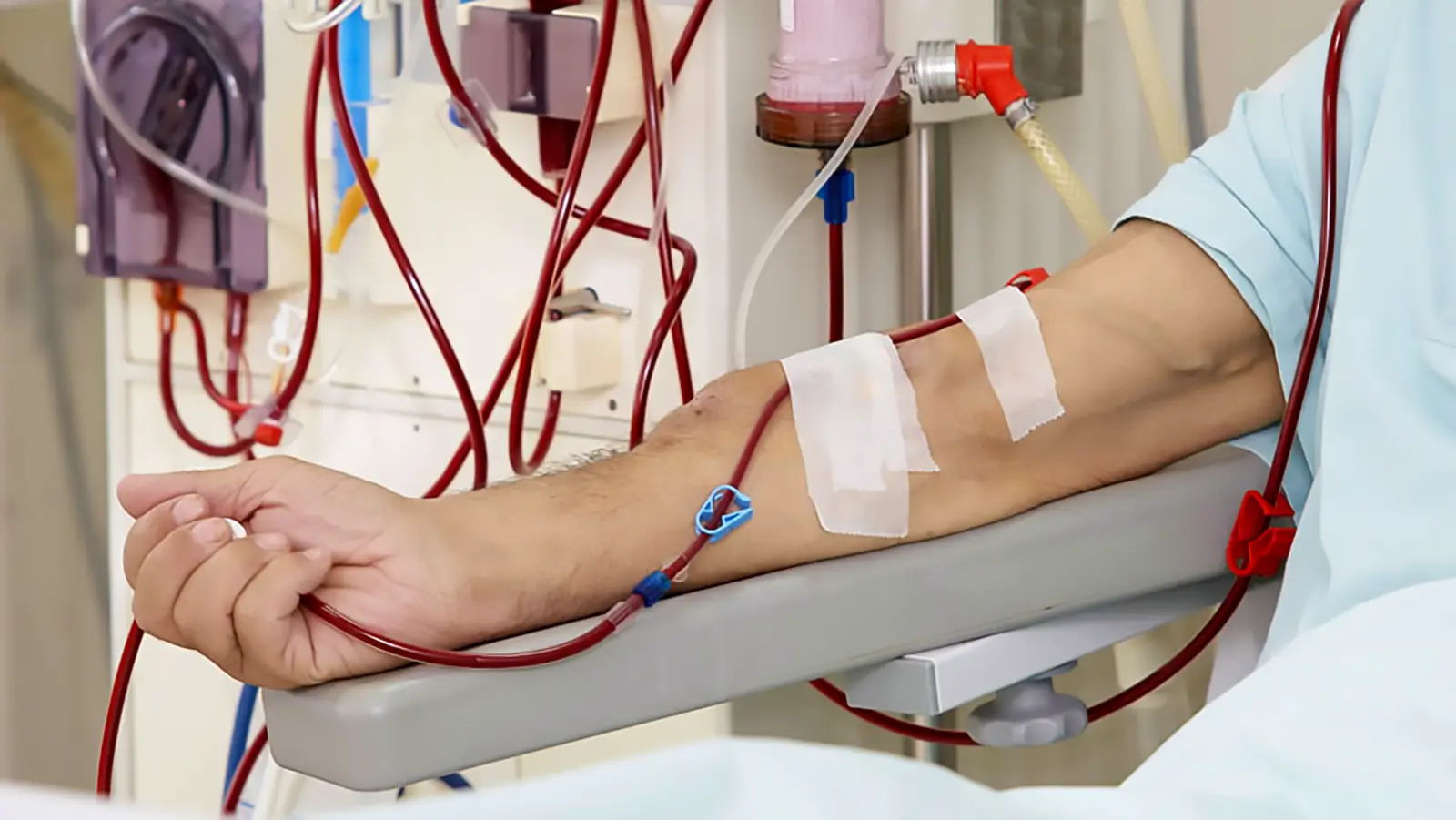
Kidney disease.
Why weight gain affects kidneys is largely unknown. There are theories but so far there is no clear answer. It might be a consequence of increased inflammation and oxidative stress, insulin resistance, and hypertension (Kovesdy et al., 2017). As fat goes everywhere it will go to the kidney as well and will create damage by raising inflammation. It is known as a fatty kidney (Foster et al., 1979). The problem with kidneys is that unlike the liver they cannot regenerate themselves. Once the damage is done it will remain for the rest of the life. Having excessive weight will increase the damage and losing weight afterward will not reverse the damage that has already been done. It will also increase the risk of kidney cancer.
Obesity also creates inflammation in the body as a general rule. This means that if we are obese we will have to take a much higher level of antioxidant-rich anti-inflammatory food than someone who is not because we will have a higher level of chronic inflammation that will have a cascading effect and none of them are good. From cancer risk to cardiovascular risk. When inflammation rises the response of the body will be to increase cortisol production by the adrenal glands as it is the main anti-inflammatory hormone of the body. But then that can create high cortisol levels or in other words Cushing’s syndrome. Cortisol is also a stress hormone that puts the body in flight or fight mode and is correlated to different conditions from insomnia, anxiety, and also it is a catabolic hormone that will catabolize muscle mass.
By now you understand that this is just the list of diseases that are directly associated with just excessive weight gain. In real life, this list should be widened because most people that are obese are not on the whole food plant-based nutrient-rich anti-inflammatory, antioxidant-rich, nutrient-dense diet.
References:
- Ylli, D. (2022, September 6). Endocrine Changes in Obesity. Endotext – NCBI Bookshelf. https://www.ncbi.nlm.nih.gov/books/NBK279053/
- Picon-Ruiz, M., Morata-Tarifa, C., Valle-Goffin, J. J., Friedman, E. R., & Slingerland, J. M. (2017). Obesity and adverse breast cancer risk and outcome: Mechanistic insights and strategies for intervention. CA: a cancer journal for clinicians, 67(5), 378–397. https://doi.org/10.3322/caac.21405
- King, L. K., March, L., & Anandacoomarasamy, A. (2013). Obesity & osteoarthritis. The Indian journal of medical research, 138(2), 185–193.[PuMed]
- Scacchi, M., Pincelli, A. I., & Cavagnini, F. (1999). Growth hormone in obesity. International journal of obesity and related metabolic disorders : journal of the International Association for the Study of Obesity, 23(3), 260–271. https://doi.org/10.1038/sj.ijo.0800807
- Almandoz, J. P., Singh, E., Howell, L. A., Grothe, K., Vlazny, D. T., Smailovic, A., Irving, B. A., Nelson, R. H., & Miles, J. M. (2013). Spillover of Fatty acids during dietary fat storage in type 2 diabetes: relationship to body fat depots and effects of weight loss. Diabetes, 62(6), 1897–1903. https://doi.org/10.2337/db12-1407
- Møller, N., Jørgensen, J. O., Abildgård, N., Orskov, L., Schmitz, O., & Christiansen, J. S. (1991). Effects of growth hormone on glucose metabolism. Hormone research, 36 Suppl 1, 32–35.[PubMed]
- Engin A. B. (2017). What Is Lipotoxicity?. Advances in experimental medicine and biology, 960, 197–220. https://doi.org/10.1007/978-3-319-48382-5_8
- King, L. K., March, L., & Anandacoomarasamy, A. (2013). Obesity & osteoarthritis. The Indian journal of medical research, 138(2), 185–193.[PubMed]
- Schwartz, A. R., Patil, S. P., Laffan, A. M., Polotsky, V., Schneider, H., & Smith, P. L. (2008). Obesity and obstructive sleep apnea: pathogenic mechanisms and therapeutic approaches. Proceedings of the American Thoracic Society, 5(2), 185–192. https://doi.org/10.1513/pats.200708-137MG
- Kovesdy, C. P., Furth, S. L., Zoccali, C., & World Kidney Day Steering Committee (2017). Obesity and Kidney Disease: Hidden Consequences of the Epidemic. Canadian journal of kidney health and disease, 4, 2054358117698669. https://doi.org/10.1177/2054358117698669
- Foster, M. C., Hwang, S. J., Porter, S. A., Massaro, J. M., Hoffmann, U., & Fox, C. S. (2011). Fatty kidney, hypertension, and chronic kidney disease: the Framingham Heart Study. Hypertension (Dallas, Tex. : 1979), 58(5), 784–790. https://doi.org/10.1161/HYPERTENSIONAHA.111.175315
- Abraham, S. B., Rubino, D., Sinaii, N., Ramsey, S., & Nieman, L. K. (2013). Cortisol, obesity, and the metabolic syndrome: a cross-sectional study of obese subjects and review of the literature. Obesity (Silver Spring, Md.), 21(1), E105–E117. https://doi.org/10.1002/oby.20083
- Pasquali, R., Patton, L., & Gambineri, A. (2007). Obesity and infertility. Current opinion in endocrinology, diabetes, and obesity, 14(6), 482–487. https://doi.org/10.1097/MED.0b013e3282f1d6cb
- Manrique-Acevedo, C., Chinnakotla, B., Padilla, J., Martinez-Lemus, L. A., & Gozal, D. (2020). Obesity and cardiovascular disease in women. International journal of obesity (2005), 44(6), 1210–1226. https://doi.org/10.1038/s41366-020-0548-0
Related Posts













Do you have any questions about nutrition and health?
I would love to hear from you and answer them in my next post. I appreciate your input and opinion and I look forward to hearing from you soon. I also invite you to follow us on Facebook, Instagram, and Pinterest for more diet, nutrition, and health content. You can leave a comment there and connect with other health enthusiasts, share your tips and experiences, and get support and encouragement from our team and community.
I hope that this post was informative and enjoyable for you and that you are prepared to apply the insights you learned. If you found this post helpful, please share it with your friends and family who might also benefit from it. You never know who might need some guidance and support on their health journey.
– You Might Also Like –

Pesticides in Food, Exposure in The Standard American Diet- 80 Percent From Meat

Calorie restriction, Autophagy, Longevity, and Muscle loss

Homemade Natural Mouthwash: Proven, Stronger & Less Toxic

Raw food diet- The evolutionary perspective

Vitamin D deficiency- Risk Factors

Protein Requirements- Inconvenient truth

Alkaline water- Health benefits and risks

Air Pollution Exposure- Health Risks and Prevention Strategies
Learn About Nutrition
Milos Pokimica is a doctor of natural medicine, clinical nutritionist, medical health and nutrition writer, and nutritional science advisor. Author of the book series Go Vegan? Review of Science, he also operates the natural health website GoVeganWay.com
Medical Disclaimer
GoVeganWay.com brings you reviews of the latest nutrition and health-related research. The information provided represents the personal opinion of the author and is not intended nor implied to be a substitute for professional medical advice, diagnosis, or treatment. The information provided is for informational purposes only and is not intended to serve as a substitute for the consultation, diagnosis, and/or medical treatment of a qualified physician or healthcare provider.NEVER DISREGARD PROFESSIONAL MEDICAL ADVICE OR DELAY SEEKING MEDICAL TREATMENT BECAUSE OF SOMETHING YOU HAVE READ ON OR ACCESSED THROUGH GoVeganWay.com
NEVER APPLY ANY LIFESTYLE CHANGES OR ANY CHANGES AT ALL AS A CONSEQUENCE OF SOMETHING YOU HAVE READ IN GoVeganWay.com BEFORE CONSULTING LICENCED MEDICAL PRACTITIONER.
In the event of a medical emergency, call a doctor or 911 immediately. GoVeganWay.com does not recommend or endorse any specific groups, organizations, tests, physicians, products, procedures, opinions, or other information that may be mentioned inside.
Editor Picks –

Cancer Editor Picks Phytochemicals
Anticancer Power of Fruits and Vegetables: In Vivo and Clinical Evidence
Some vegetable extracts rival leading chemotherapy drugs and at the same time target multiple different types of cancer cells.

Antioxidants Editor Picks ORAC
Essential Oils as Antioxidant Supplements: Rules and Strategies
Food-grade essential oils can be a convenient and consumer-friendly strategy for optimizing the antioxidant value and ORAC scores of our diet.

Antioxidants Editor Picks ORAC
Antioxidant-Rich Diet: General Rules and Strategies
There are easy and cost-effective strategies for optimizing the antioxidant value of our diet.

Antioxidants Editor Picks ORAC
Understanding ORAC Values: Antioxidant Levels in Foods
When your main source of antioxidants is coffee, you know that you have a serious problem.

Antioxidants Editor Picks ORAC
Astaxanthin Benefits: World’s Most Powerful Natural Antioxidant
Astaxanthin is the most powerful natural and universal antioxidant (both oil and water-soluble) known to science. It accumulates in tissues and It can never turn itself into a pro-oxidant.

Antioxidants Editor Picks ORAC Phytochemicals
Antioxidants: Understanding the Basics
There are no phytochemicals or antioxidants in animal products. On average, plant foods contain more than 60 times as many antioxidants as animal-based foods.

Editor Picks Vegan Diet
Nutrient Deficiencies in Vegan Diet: Prevention Strategies
There are nine common nutrient deficiencies on the population scale affecting people eating a plant-based diet. If not corrected on time some deficiencies have terrible and non-treatable consequences.

Editor Picks Optimal Diet
Micronutrient Deficiency in Standard American Diet: Optimization Strategies
Nutrition profile of our modern meat, sugar, processed food diet is completely incongruent with our evolution resulting in severe micronutrient deficiency.

Editor Picks Phytochemicals
Phytochemicals: Understanding the Basics
Every single phytochemical that exists has a biological action in the human body. Every single one from millions of different phytochemicals.

Editor Picks Milk Optimal Diet
Milk and Dairy: Health Risk Correlations
Known associations with milk and dairy consumption are infertility, ovarian and breast cancer, leukemia, diabetes type 1, autism, arteriosclerosis, cataract, rheumatoid arthritis, multiple sclerosis, hyperactivity, congestion, pimples, and more…
Cancer Editor Picks Protein
Complete Protein: IGF-1 Signaling in Cancer Formation
When you eat animal protein you have four times the chance to develop all types of cancer. When you smoke you have a four-time chance to develop lung cancer.

Cancer Editor Picks Protein
The Anatomy of Cancer- Health risk correlations
About 2% of cancers are by medicine considered to be purely caused by genetic factors. The same range as within the animal kingdom. You haven’t been told the whole truth.
Milos Pokimica is a health and nutrition writer and nutritional science advisor. Author of the book series Go Vegan? Review of Science, he also operates the natural health website GoVeganWay.com
Latest Articles –

Calorie Restriction Longevity
How to Fast: Fasting Foods That Won’t Break Autophagy
Autophagy. Have you ever wondered what happens to the cells in your body when they die or get damaged? Do they just pile up and create problems, or do they get disposed of somehow? The answer is that your body…

Dental Health Prevention
Sweets Teeth Sensitivity & Pain: Quick Fix & Lasting Solution
A quick and easy fix for pain relief is clove essential oil, a powerful antioxidant and pain reliever that can help with gum disease and toothache.

Beans
Green Beans: Nutrition and Health Benefits
Green beans are low in calories and rich in natural compounds that can help you control your blood sugar, lower your cholesterol, and fight off free radicals.

Raw food diet Vegan Diet
Can You Eat Mushrooms Raw: Health Risks, Nutrition & Safety
Mushrooms have heat-sensitive toxins like hydrazine or agaritine, and cell walls made out of chitin that cannot be digested well by humans.
Vegan Diet
Are Fish Animals? A Cultural Perspective
In some cultures, fish meat is not considered to be meat, and fish is allowed even during fast.

Dental Health Prevention
Homemade Natural Mouthwash: Proven, Stronger & Less Toxic
Homemade natural mouthwash is stronger than chlorhexidine, less toxic and if swallowed might give you some nausea but also a high burst in ORAC value.

Dental Health Prevention
How to Stop Tooth Decay: Symptoms, Causes & Prevention
Sugar consumption is the main cause of cavities and tooth decay, combined with mineral deficiencies especially magnesium, zinc, copper and trace elements.

Antioxidants Superfoods
Amla: Proven Benefits, Nutrition And Clinical Significance
Amla is one of the world’s most powerful antioxidants with a ORAC score of 261,530. It is a rich source of phytochemicals that have various health benefits.
Top Health News — ScienceDaily
- New MRI breakthrough reveals the brain and eye like never beforeon July 10, 2026
Scientists have redesigned a key piece of MRI hardware using metamaterials, allowing existing scanners to produce clearer images of difficult-to-see parts of the body in less time. The breakthrough could improve diagnoses, make scans more comfortable, and open the door to new medical imaging and treatment applications.
- This frog bacterium wiped out cancer tumors in mice with a single doseon July 10, 2026
A naturally occurring bacterium from amphibian intestines completely eliminated colorectal tumors in mice with a single treatment by both attacking cancer cells and activating the immune system. The findings point to a promising new type of cancer therapy that could one day work against many solid tumors.
- Scientists found a longevity diet that helped mice eat more and lose faton July 10, 2026
Scientists found that a modified Mediterranean-style diet with low protein and just enough methionine helped mice live healthier lives while reducing body fat and frailty. Human data also linked lower animal protein intake to lower rates of obesity and Type 2 diabetes, suggesting the approach could benefit people as well.
- Scientists just debunked a dangerous baby rattlesnake mython July 10, 2026
A new study debunks the long-standing claim that baby rattlesnakes are more dangerous than adults. Researchers found that young rattlesnakes can control their venom just like adults, while adult snakes usually inject much more venom and cause more serious bites. The team also uncovered how the myth spread through decades of inaccurate news reports and misleading quotes from trusted sources.
- A hidden immune backup system could supercharge mRNA cancer vaccineson July 9, 2026
Researchers found that mRNA cancer vaccines can recruit an unexpected immune cell to launch powerful tumor-fighting responses, overturning a long-held assumption about how the vaccines work. The discovery could lead to more effective cancer vaccines and help scientists tailor treatments for better patient outcomes.
- A vitamin A discovery is changing what scientists know about visionon July 9, 2026
A surprising discovery is reshaping scientists’ understanding of how humans develop sharp central vision before birth. Instead of blue cone cells migrating away from the retina’s center, the study found they transform into red and green cones under the influence of vitamin A-related signals and thyroid hormones. The findings could improve lab-grown retinal tissue and lay the groundwork for future cell therapies to restore vision lost to age-related eye diseases.
- The Ozempic and Wegovy mistake sending thousands to poison controlon July 9, 2026
Poison control calls involving semaglutide (Ozempic and Wegovy) soared after the drug was approved for weight management, with researchers linking the increase to accidental dosing mistakes rather than intentional misuse. Simple education about proper weekly dosing and gradual dose increases could help prevent many of these avoidable incidents.
PubMed, #vegan-diet –
- Comparative Analysis of Diet Quality, Iron Intake, and Supplementation Among Vegan and Omnivorous Amateur Runners Living in Urban Areason July 10, 2026
Plant-based diets, including vegan and vegetarian patterns, are gaining popularity among physically active individuals, including amateur runners. While such diets may offer health benefits, they also carry a risk of inadequate intake of key nutrients, among which iron plays a crucial role. This study compared diet quality, iron intake, and dietary supplementation among vegan, lactovegetarian, and omnivorous amateur runners in Warsaw, Poland. One hundred runners (52 males, 48 females; aged…
- Are Vegetarian and Vegan Diets Associated With Eating Disorder Symptoms? A Systematic Review and Meta-Analysison July 8, 2026
OBJECTIVE: To synthesize the evidence on the associations between vegetarian and vegan diets (VVDs) and eating disorder (ED) symptoms compared with omnivorous diets across the lifespan.
- Does creatine supplementation improve strength and power in physically active individuals on a vegan diet? a randomized, triple-blind, placebo-controlled trialon July 2, 2026
CONCLUSION: Four weeks of creatine supplementation in individuals following a vegan diet enhances muscle strength and lower-body muscular power. Longer-term studies are needed to confirm the effectiveness and safety of creatine supplementation in this population.
- Comparative Efficacy of Intranasal, Intramuscular, and Intravenous Vitamin B12 Therapy for Hematological Recovery in Vitamin B12 Deficiency Anemia: A Randomized Controlled Trialon July 2, 2026
Vitamin B12 deficiency causes megaloblastic anemia and ineffective hematopoiesis. While intramuscular administration remains standard, intravenous and intranasal alternatives are increasingly used. Rigorous comparative data on hematological efficacy across routes remain limited. We thus aimed to compare intranasal, intramuscular, and intravenous vitamin B12 therapy for hematological recovery in vitamin B12 deficiency anemia, and to identify independent predictors of treatment response. In […]
- Social Identity and Wellbeing of Australian Vegan Men: A Qualitative Interview Studyon June 30, 2026
CONCLUSION: Australian vegan men navigated their social identities through out-group dynamics involving masculinity, ethical commitments and community integration, and in-group dynamics marked by dietary boundary negotiation and solidarity with vegan communities. However, they also faced social isolation and strained relationships. SO WHAT?: Their experiences reflected identity negotiation processes shaped by moral values, subgroup tensions and the importance of supportive social […]
Random Posts –

Longevity Optimal Diet Vegan Diet
B12 Deficiency and Cognitive Decline: Homocysteine Optimization Strategies
Vitamins that regulate homocysteine levels are B12, folate, and B6. Most non-vegans get enough B12 but not enough folate while vegans get more folate but do not have any B12 if not supplemented.

Editor Picks Optimal Diet Vitamin D
Vitamin D- More than just your bones
Vitamin D is not a vitamin. It is a prohormone, a steroid with a hormone-like activity that regulates about 3% of the human genome.

Coffee Toxicity
Coffee benefits– Not without the risks
Do we think caffeine is something good for our brain or bad or neutral?
What does the actual caffeine do?
Dental Health Prevention
Sweets Teeth Sensitivity & Pain: Quick Fix & Lasting Solution
A quick and easy fix for pain relief is clove essential oil, a powerful antioxidant and pain reliever that can help with gum disease and toothache.

Optimal Diet ORAC
Home oil extraction- The secret technique of nutrient density
Processing of food (home oil extraction) can also be used in reverse for increasing the nutritional density and profile of the food.
Allopathic Medicine Editor Picks Optimal Diet
The McGovern Report- Special Interest and The Suppression of Science
In 1977 the push for a change of Dietary Guidelines (McGovern Report) to more plant-based vegan one had been introduced to U.S. Congress.
Raw food diet Vegan Diet
Can You Eat Mushrooms Raw: Health Risks, Nutrition & Safety
Mushrooms have heat-sensitive toxins like hydrazine or agaritine, and cell walls made out of chitin that cannot be digested well by humans.
Cancer Editor Picks Phytochemicals
Anticancer Power of Fruits and Vegetables: In Vivo and Clinical Evidence
Some vegetable extracts rival leading chemotherapy drugs and at the same time target multiple different types of cancer cells.
Antioxidants Editor Picks ORAC
Antioxidant-Rich Diet: General Rules and Strategies
There are easy and cost-effective strategies for optimizing the antioxidant value of our diet.

Editor Picks Optimal Diet
Carnism- The psychology of meat consumption
Meat-eating is the culture that is learned. Actual carnivores would eat any meat no matter what it is, including carrion. In our system, we would eat only a few animals that we deem as food.
Featured Posts –
Editor Picks Optimal Diet Protein
High Protein Diet- Health Risk Correlations
Scarcity is the rule of protein in nature. In evolutionary terms, anthropologists have proven that hominins lived an average of 15 to 25 grams of protein a day. In the modern western type of high-protein diet we would consume that…

Allopathic Medicine Cancer Editor Picks
Cancer, The Forbidden Cures-Rife machine, Historical review
The recovery rate for patients that have non-treatable cancer and were declared terminally ill by utilizing Rife Machine resonant technology was 100%.

Editor Picks Inflammation
The humans omnivores dilemma- Meat consumption, probiotic bacteria, inflammation, and the gut
Are humans omnivores in a true anatomical sense? There is a fundamental difference in the way the digestive tract works in plant vs meat-eating species.

Editor Picks Optimal Diet
Processed Food: Understanding the Risks
Processed food means that something from whole food is removed, usually fiber and something is added, usually fat, sugar, salt, and msg.

Cancer Editor Picks Toxicity
Pesticide Exposure in Children: Real-Life Exposure Tests
Children and especially pregnant women are more vulnerable to pesticide exposure. If we analyze real-world exposure levels in real-life scenarios, what would the result be?
Cancer Editor Picks Phytochemicals
Anticancer Power of Fruits and Vegetables: In Vivo and Clinical Evidence
Some vegetable extracts rival leading chemotherapy drugs and at the same time target multiple different types of cancer cells.
Editor Picks Milk Optimal Diet
Milk and Dairy: Health Risk Correlations
Known associations with milk and dairy consumption are infertility, ovarian and breast cancer, leukemia, diabetes type 1, autism, arteriosclerosis, cataract, rheumatoid arthritis, multiple sclerosis, hyperactivity, congestion, pimples, and more…
Editor Picks Vegan Diet
Nutrient Deficiencies in Vegan Diet: Prevention Strategies
There are nine common nutrient deficiencies on the population scale affecting people eating a plant-based diet. If not corrected on time some deficiencies have terrible and non-treatable consequences.

Editor Picks Prevention Vegan Diet
China study- The vegan argument
China study showed that there is no heart disease or cancer or diabetes in undeveloped rural communities in the world with starch-based vegan diets.

Editor Picks Optimal Diet Protein
Protein Requirements- Inconvenient truth
When anthropologist studies showed that hominins lived on average of 15 to 20 grams of protein a day there was a so-called a “Great protein fiasco” back in the 1970s.
Latest from PubMed, #plant-based diet –
- Comparative Analysis of Diet Quality, Iron Intake, and Supplementation Among Vegan and Omnivorous Amateur Runners Living in Urban Areasby Gabriela Lewandowska on July 10, 2026
Plant-based diets, including vegan and vegetarian patterns, are gaining popularity among physically active individuals, including amateur runners. While such diets may offer health benefits, they also carry a risk of inadequate intake of key nutrients, among which iron plays a crucial role. This study compared diet quality, iron intake, and dietary supplementation among vegan, lactovegetarian, and omnivorous amateur runners in Warsaw, Poland. One hundred runners (52 males, 48 females; aged…
- Effects of increasing soybean meal in late nursery, grower, and finishing pig dietsby Jamil E G Faccin on July 10, 2026
Six experiments were conducted to determine the effects of increasing soybean meal (SBM) in late nursery and finishing pig diets on growth performance, fecal characteristics, and carcass traits. In Exp. 1, 266 pigs (initially 10.1 ± 0.17 kg) were randomly assigned to one of four corn-based diets with SBM levels of 25.0, 28.9, 32.5, or 36.2%. In Exp. 2, 340 pigs (initially 13.5 ± 0.18 kg) were randomly assigned to one of five corn-based diets with SBM levels of 25.0, 28.9, 32.5, 36.2, or […]
- Preserving Tradition, Preventing Cancer: A Narrative Review of the Traditional Mexican Diet as a Framework for Cancer Risk Reductionby Isaura Del Valle-Domínguez on July 10, 2026
The Traditional Mexican Diet (TMexD) is a culturally rooted, plant-forward dietary pattern derived from Mesoamerican agriculture and culinary practice, built on minimally processed staples-maize-based preparations, legumes, vegetables, fruits, and herbs. Characteristic techniques such as nixtamalization and fermentation alter starch structure, mineral availability, and gut microbial activity. Through these effects, the pattern shapes metabolic responses relevant to carcinogenesis. This […]
- Dietary pine pollen induces masculinization in Nile tilapia (Oreochromis niloticus, L. 1758) by modulating sex-biased gene expression and steroid hormone profilesby Ivan Abaho on July 9, 2026
CONCLUSION: These findings imply that PP induces female-to-male sex change in Nile tilapia by disrupting the expression of sex-biased genes and, consequently, the androgen-to-estrogen balance. However, further studies are required to enhance the androgenic potency of PP.
- Being eco-sustainable eaters: the role of chronotype and HEXACO personality traitsby Federica Scarpina on July 9, 2026
CONCLUSION: Both chronobiology and personality traits may significantly influence an individual’s inclination toward eco-sustainable dietary choices. The intrinsic characteristics of Agreeableness and Openness to Experience, but not those associated with Honesty-Humility and Extraversion, may facilitate individuals in addressing the contextual challenges of adopting an eco-sustainable diet.
- A path to sustainable and healthy diets: modeling ovo-lacto-vegetarian food-based dietary guidelinesby Lisa Sturm on July 9, 2026
INTRODUCTION: The development of healthy and sustainable food-based dietary guidelines (FBDGs) is an essential measure to support the transformation to sustainable and resilient food systems. Shifting to more sustainable and healthy plant-based diets can benefit both human and planetary health, provided these diets are nutritionally adequate, healthy, environmentally friendly, and culturally acceptable.